
Έρευνες πανεπιστημίων
-
Implementation of a Defecation Posture Modification Device: Impact on Bowel Movement Patterns in Healthy Subjects
Περιεχόμενο με δυνατότητα σύμπτυξης
Abstract
GOALS: The goal of this study was to evaluate the influence of defecation postural modification devices (DPMDs) on normal bowel patterns.
Background
The introduction of DPMDs has brought increased awareness to bowel habits in western populations.
Materials and Methods :
A prospective crossover study of volunteers was performed that included real-time collection of data regarding bowel movements (BMs) for 4 weeks (first 2 wk without DPMD and subsequent 2 wk with DPMD). Primary outcomes of interest included BM duration, straining, and bowel emptiness with and without DPMD use.
-
Results
In total, 52 participants (mean age, 29 y and 40.1% female) were recruited for this study. At baseline 15 subjects (28.8%) reported incomplete emptying, 23 subjects (44.2%) had increased straining, and 29 subjects (55.8%) noticed blood on their toilet paper in the past year. A total of 1119 BMs were recorded (735 without DPMD and 384 with DPMD).
Utilizing the DPMD resulted in increased bowel emptiness (odds ratio, 3.64; 95% confidence interval (CI), 2.78-4.77) and reduced straining patterns (odds ratio, 0.23; 95% CI, 0.18-0.30). Moreover, without the DPMD, participants had an increase in BM duration (fold increase, 1.25; 95% CI, 1.17-1.33).
-
Conclusions:
DPMDs positively influenced BM duration, straining patterns, and complete evacuation of bowels in this study.
Comparison of Straining During Defecation in Three Positions
Results and Implications for Human Health
-
DOV SIKIROV, MD
The aim of the study was to compare the straining forces applied when sitting or squatting during defecation. Twenty-eight apparently healthy volunteers (ages 17–66 years) with normal bowel function were asked to use a digital timer to record the net time needed for sensation of satisfactory emptying while defecating in three alternative positions: sitting on a standard-sized toilet seat (41– 42 cm high), sitting on a lower toilet seat (31–32 cm high), and squatting.
They were also asked to note their subjective impression of the intensity of the defecation effort. Six consecutive bowel movements were recorded in each position. Both the time needed for sensation of satisfactory bowel emptying and the degree of subjectively assessed straining in the squatting position were reduced sharply in all volunteers compared with both sitting positions (P < 0.0001). In conclusion, the present study confirmed that sensation of satisfactory bowel emptying in sitting defecation posture necessitates excessive expulsive effort compared to the squatting posture.
-
KEY WORDS: straining; sitting; squatting; defecation posture.
The straining forces applied during defecation may be very significant in the etiology of pathological conditions. While squatting for defecation continues to be the principal position in Asia and Africa, Western populations have become accustomed to sitting on toilet seats.
Little is known about any differences in the straining forces between these two positions. In the present study, the time needed for sensation of satisfactory bowel emptying was recorded while the subjects sat on toilet seats of two different heights as well as while they squatted. They also recorded their subjective impressions of the intensity of straining needed to empty the bowel in each of these three positions.
-
MATERIALS AND METHODS
Twenty-eight volunteers (14 males, 14 females, age range 17– 66 years) with apparently normal bowel function agreed to take part in the study.
Individuals who were unable to assume a squatting posture for any reason were excluded as were those who had less than one or more than three bowel movements per day in order that the cohort would represent the majority (as 95%) of a total population (2). The volunteers were instructed to interrupt the trial if they suffered from diarrhea and to resume when it had been resolved.
Upon questioning for type of diet, it was found that it varied, very significantly, from person to person sometimes as can be expected. The volunteers were instructed not to change their usuual diets and defecation habits. They were supplied with a digital timer with a start/stop function for counting seconds and minutes and were asked to record the net amount of time that had been needed for sensation of satisfactory bowel emptying on a predesigned form.
Specifically, they were instructed to press the start button when they first began to strain and to press the stop button when they had finished emptying their bowels. The same form included a questionnaire for subjective assessment of any difficulties in defecation graded from very easy to very difficult.
Four forms per participant had been prepared for the original four stages of the study: the completed form was exchanged for the following one to avoid comparisons of entries and possible bias.
• The first stage involved registering the time that had elapsed during rectal emptying with the subject seated on a regular toilet seat (41–42 cm from the base and including the seat).
• The second stage was the same as the first but with the subject’s feet resting on a 10-cm high footstool, which reduced the height of the toilet seat to 31–32 cm.
• The third stage was supposed to have been the same as the second but with the use of a 15-cm high footstool, thus reducing the height of toilet bowl to 26–27 cm: this stage was abandoned when four consecutive volunteers refused to complete the required number of defecation trials because of the extreme discomfort of defecating in this position.
In the fourth stage, the subject defecated while in a squatting posture (a flat container was supplied). The volunteers were instructed to record six consecutive bowel movements in each position.
The number six was chosen arbitrarily, taking into account that although a greater number would more accurately reflect the whole picture, it should not be so numerous as to interfere with compliance of the volunteers to complete the tasks. Prior to this study all volunteers routinely used a seated posture for defecation.
-
Statistical Analysis
Comparison between the averages of measured time and subjective assessment of difficulty in defecating in different postures was done by the Wilcoxon rank test. Comparison between the different postures was based on P = 0.017 (0.05/3) according to the Bonferroni correction.
The subjective assessment of difficulty in defecating was estimated as: 0 = very easy, 1 = easy, 3 = moderate, 5 = difficult. The sum of answers was divided by 3 in order to arrive at the scale 0–10 (10, most difficult; 0, easiest).
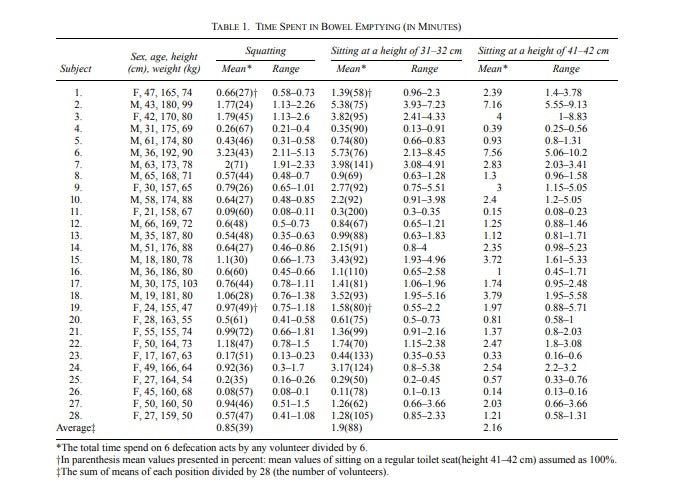
Table 1
Results
The results are summarized in Tables 1 and 2 and Figures 1 and 2. The study revealed that the subjects had different patterns of bowel emptying (Table 1).
-
For example, volunteer 26 characteristically had very rapid bowel movements that lasted only a few seconds, while volunteer 6 usually took several minutes. Irrespective of the differences in patterns, all the subjects registered a sharp reduction of time necessary for sensation of satisfactory bowel emptying in the squatting posture compared to either of the sitting positions (Table 1, Figure 1).
The subjective assessment of the difficulty of defecation revealed the squatting posture as easiest for sensation of satisfactore bowel emptying compared with any sitting defecation posture (Table 2, Figure 2).
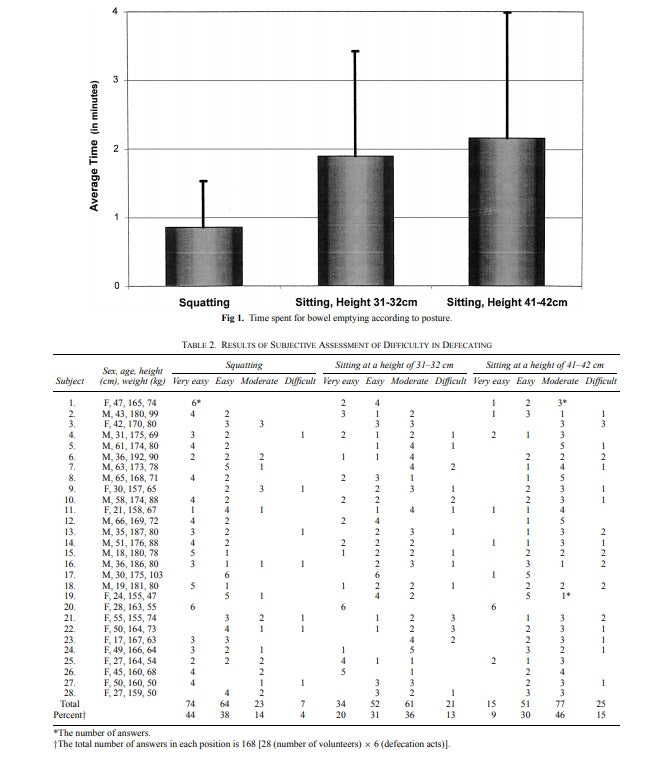
Table 2
Statistical difference
The statistical difference for both the averages of measured time and subjective assessment of intensity of defecation effort between squatting and any sitting posture was highly significant (P < 0.0001). Most of the volunteers also registered a reduction in the time needed for sensation of satisfactory bowel emptying while seated on the lower seat compared to the standardsized one (P = 0.002). The tendency to spend less time in sensation of satisfactory bowel emptying in the former position was also reflected in the subjective assessment of difficulty in defecating (P = 0.046)
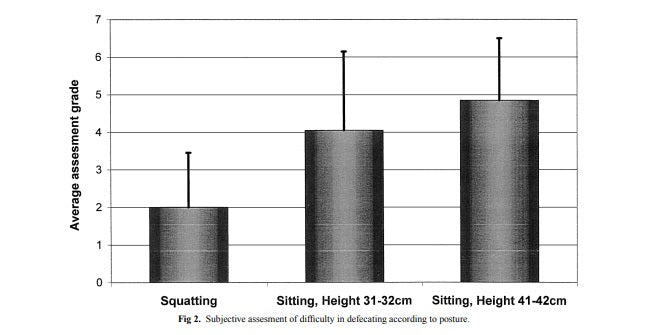
table 3
Πιο αναλυτικά
-
However, six volunteers (21%) spend more time for sensation of satisfactory bowel emptying while seated on the lower seat compared to the standard-sized one. There was no statistical correlation between subjective assessment and the measured time needed for sensation of satisfactory bowel emptying. An occasional finding was the direct correlation between the weight of volunteers and the measured time necessary for sensation of satisfactory bowel emptying (ρ > 0.35 by Spearman correlation test).
Discussion
-
The uniformity of results described in this paper can be explained by a anatomophysiological factor common to humans, the rectoanal angle, which is straightened with hip flexing.
The angle between the rectum and the anal canal varies from one individual to another (graded 64– 134) (3) and is a major factor in continence for solid rectal content (4). In his radiological study, Tagart showed that the rectoanal angle straightens with fully flexed hips—corresponding to the squatting position assumed for defecation—and converts the rectoanal outlet into a straight canal, thereby facilitating rectal emptying (5).
The results of the present study are in excellent agreement with this line of thinking and may be summarized as follows: the greater the hip flexion, the straighter the rectoanal canal and, accordingly, the less strain required emptying the bowels.
The only deviation from this rule in the present study cohort was seen in the six volunteers (Subjects 7, 11, 16, 23, 24, and 28) who had reported more straining for emptying the rectum while sitting on the lower toilet seat. It can be speculated that hip flexion, which is usually greater in this posture than when seated on a regular toilet seat, was not sufficient to straighten the rectoanal canal and reduce the straining in these subjects while the unusual position of sitting on a toilet seat 31– 32 cm high had a strong influence on these volunteers’ expressing the need for more straining than they had required while sitting on a regular toilet seat.
The attempt to achieve more straining reduction in sitting posture by even more reduction of height of toilet seat and accordingly more hip flexing was not successful. As noted above, four consecutive volunteers refused to defecate on a toilet seat 26–27 cm high because of unacceptable discomfort. All volunteers, independently of variables such as diet, length of feces evacuation, age, height, weight, and sex, needed significantly less time for feces evacuation in the squatting posture than in any sitting posture.
This phenomenon, characteristic of 100% of volunteers, excludes the possibility that the additional time spent on defecation in the sitting posture is an innocent factor lacking any significance. Moreover, in sitting postures, the volunteers spent on average 1.9–2.1 min to empty the rectum. It is too short a time for reading the paper or just sitting, but it is too long compared with the 0.85 min spent on sensation of satisfactory bowel emptying in squatting posture. The extra time spent in the sitting posture is necessary for excessive straining in order to push the feces through almost right rectoanal angle, while in the squatting posture significantly less straining is necessary as the feces are pushing out along the open outlet due to straightening of the rectoanal junction.
The above arguments are in agreement with the volunteers’ subjective assessment, which determined defecation is “very easy” in 44% in the squatting posture, while this was as in 9–20% in the sitting postures (Table 2), generally assessing the sitting postures 2–2.5 time more difficult than the squatting posture (Figure 2).
From elementary mechanics it is well known that any system exposed to excessive pressures ultimately sustains injury (6). Historically, man has squatted in order to defecate (7), and the practice continues today in underdeveloped countries (8). The widespread use of a sitting toilet in the Western world began during the 19th century when sewage systems were developed to improve sanitation as cities grew (9). In the middle of the 20th century, a group of physicians working in rural Africa were surprised by the near absence of hemorrhoids, constipation, hiatus hernia, and diverticulosis coli in rural black populations (10). They further found that the rarity of these problems is also characteristic for other underdeveloped countries.
Those authors attributed this finding to a high fiber diet, and studies were embarked upon to confirm this hypothesis with regard to diverticulosis coli. Following this and other publications, the Western world has taken steps to enrich their diets with edible fibers, but the prevalence of the abovementioned diseases has not changed. Moreover, several later studies on the role of low fiber diet in the etiology of diverticulosis coli could not confirm such associations (11–13).
The results of the present study can well explain the findings of Burkitt et al (10) of specific geographic distributions of the diseases mentioned: individuals residing in geographical areas with a high prevalence of these problems characteristically use sitting toilets while a low prevalence is found in areas where people characteristically use squatting toilets.
The defecation act results from a chain of events known as Valsalva maneuver and when protracted and repeated may case cardiac rhythm disturbances (14, 15), reduction of coronary (16) and cerebral (17) blood flow explaining defecation syncope and death (14, 17, 18).
The brief defecation effort in the squatting posture, as shown in this study, may prevent many cardiovascular events. In conclusion, the present study, together with the earlier data in the literature, point to the far greater expulsive effort needed for defection while seated as a being the causative factor of several medical problems.
Περιεχόμενο με δυνατότητα σύμπτυξης
ACKNOWLEDGMENTS
The author thanks Doron Comaneshter, Tel Aviv Sourasky Medical Center, for the statistical analysis and assistance.
REFERENCES
1. Gatewood WE: The mechanics of the colon. Northwest Med 29:1–7, 1930 2. Connel AM, Hilton C, Irvine G, Lennard-Jones JE, Misiewicz JJ: Variation of bowel habit in two population samples. Br Med J 2:1095–1099, 1965 3. Shorvon PJ, Mchugh S, Diamant NE, Somers S, Stevenson GW: Defecography in normal volunteers: results and implications. Gut 30:1737–1749, 1989 4. Altomare DF, Rinaldi M, Veglia A, Guglielmi A, Sallustio PL, Tripoli G: Contribution of posture to the maintenance of anal continence Int J Colorectal Dis 16:51–54, 2001 5. Tagart RE: The anal canal and rectum: their varying relationship and its effect on anal continence. Dis Colon Rectum 9:449–452, 1966 6. Timoshenko S: Theory of Elastic Stability. New York, McGraw-Hill, 1936 7. Haubruch W: Constipation. In Bockus Gastroenterology, 4th ed. J Berk (ed). Philadelphia, Saunders, 1985, p 111 8. Boles R: Constipation. JAMA 89:1766–1770, 1927 9. Singer C, Holmyard E, Hall A, Williams T: History of Technology. The Industrial Revolution 1750–1850, Oxford, Clarendon Press, 1958, pp 507–508 10. Burkitt D, Walker A, Painter N: Dietary fiber and disease. JAMA 229:1068–1074, 1974 11. Eastwood M, Smith A, Brydon W, Pritchard J: Colonic function in patients with diverticular disease. Lancet 1:1181–1182, 1978 12. Parks T, Connel A: Motility studies in diverticular disease of the colon. Gut 10:534–542, 1969 13. Weinreich J, Andersen D: Intraluminal pressure in the sigmoid colon. Patients with sigmoid diverticula and related conditions. Scand J Gastroenterol 11:581–586, 1976 14. McGuire J, Green RS, Haenstein V, Courter S, Braunstein JR, Plessinger V, Iglauer A, Noertker J: Bed pan deaths. Am Pract Dig Treatment 1:23–28, 1950 15. Schartum S: Ventricular arrest caused by the Valsalva maneuver in a patient with Adams-Stokes attacks accompanying defecation. Acta Med Scand 184:65–68, 1968 16. Benchimal A., Wang FU, Desser KB, Gartlan JL: The Valsalva maneuver and coronary arterial blood flow velocity. Ann Intern Med 77:357–360, 1972 17. Greenfield J: Transient changes in cerebral vascular resistance during the Valsalva maneuver in man. Stroke 15:76–79, 1984 18. Kapoor. W. N, Peterson J, Karpf M: Defecation syncope. Arch Intern Med 146:2377–2379, 1986